

Infertility impacts 1 in 8 women in the United States, and treating infertility can quickly become costly. Since Flow Financial Planning primarily works with early-to-mid-career women who are often grappling with big career, family, and financial decisions during their (possibly last) fertile years, any plan feels incomplete without addressing the biology and finances of fertility.
[Meg’s Note: This post was written by guest bloggers Erin Coffman and Rebecca Rosenfelt. Erin and Rebecca are data scientists professionally—they met while working together at Airbnb—and also have personal experience with this topic. Erin has a PhD in Economics, and both love applying economic principles to everyday life. Because fertility is such a numbers game, they thought a data-focused lens on the (in)fertility experience would be helpful to others. Keep in mind they are not doctors (just data nerds), so if you have questions about your specific situation, it’s best to consult a doctor. Learn more about Erin and Rebecca.]
The main points we’ll cover:
- Fertility only declines over time (womp womp)
- Getting your fertility levels tested gives you useful information
- Preserving fertility through egg freezing is cheaper now than it will be 10 years from now, so worth considering (even though it’s not a 100% guarantee)
One thing it’s important to acknowledge is that not everyone wants children — this is a very personal decision, and any route you choose to take is valid. Our goal is to lay out some financial considerations if you do think you may want kids, or if you’re not sure yet. We also tend to refer to women here, but point out that not only women have uteruses, and indeed using your uterus is not the only way to have a child.
Why test my fertility now? My mom/sister/etc. had lots of kids and no issues.
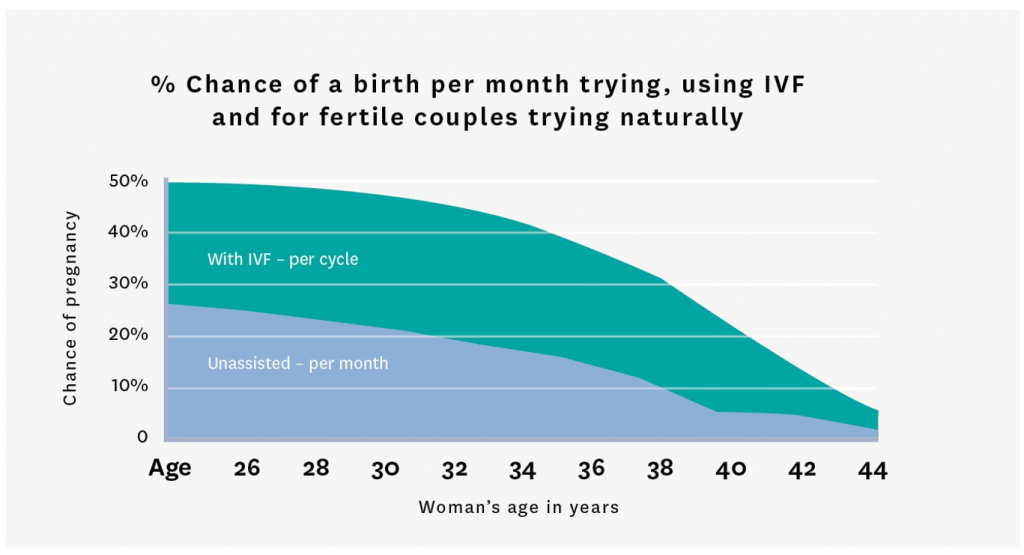
Age is the biggest predictor of fertility; as you age, your fertility only declines. This is very inconvenient, and we try to tell ourselves the decline isn’t that bad, and we look for examples of women who beat the odds.
In behavioral economics, there’s a phenomenon known as survivorship bias, wherein we focus on successes, not failures, because failures are not as visible. In other words, we are much more likely to be aware of a baby than a lack of a baby.
This is dangerous because it gives a false sense of extended fertility. We see pregnant women over 40, a Hollywood actress having twins at 45, and assume that these are common occurrences. But that’s because
we don’t see those who are unsuccessful, those who’ve given up trying, those who are on their 8th round of IVF.
We don’t know that the 45 year old may have used a donor egg. Try to be aware that what you see are exceptions, not the norm. Here is a more realistic picture (not a fun chart, we know) of average fertility outcomes over time [Meg’s note May 30, 2025: This link has since stopped working]:
What should I do first?
We recommend starting with some basic testing to get a sense of where you are on the fertility spectrum. You can ask your primary care doctor for the tests, get a referral to a fertility specialist, or even order an at-home kit from a site like ModernFertility.com (caveat: we haven’t used them and can’t vouch for this option).
Usually, doctors will look at several hormones. They may also do an ultrasound to ensure your physical structures look ok and also to count your follicles (these are the sacs on your ovaries that release eggs). This helps build a complete picture.
One hormone that may get extra focus is your AMH (anti-mullerian hormone), as this is related to your egg reserves. Women are born with all the eggs they’ll ever have, and over time the number of eggs you have left diminishes. AMH gives you a sense of how many you have left, and whether your number is typical for your age.
A low AMH doesn’t mean your eggs are of poor quality, or that you won’t be able to get pregnant naturally. Rather, it correlates with how well you’ll respond to follicular stimulation, aka IVF drugs that put your ovaries into hyperdrive to release as many eggs as possible when doing an egg freezing or IVF cycle.
Fertility treatment is a numbers game, and you generally want to start with big numbers (more on that later). A higher AMH level generally means you’ll get more eggs when stimulated with IVF drugs.
Here is a chart showing typical AMH levels by age in the general population, not just women going through fertility treatments:
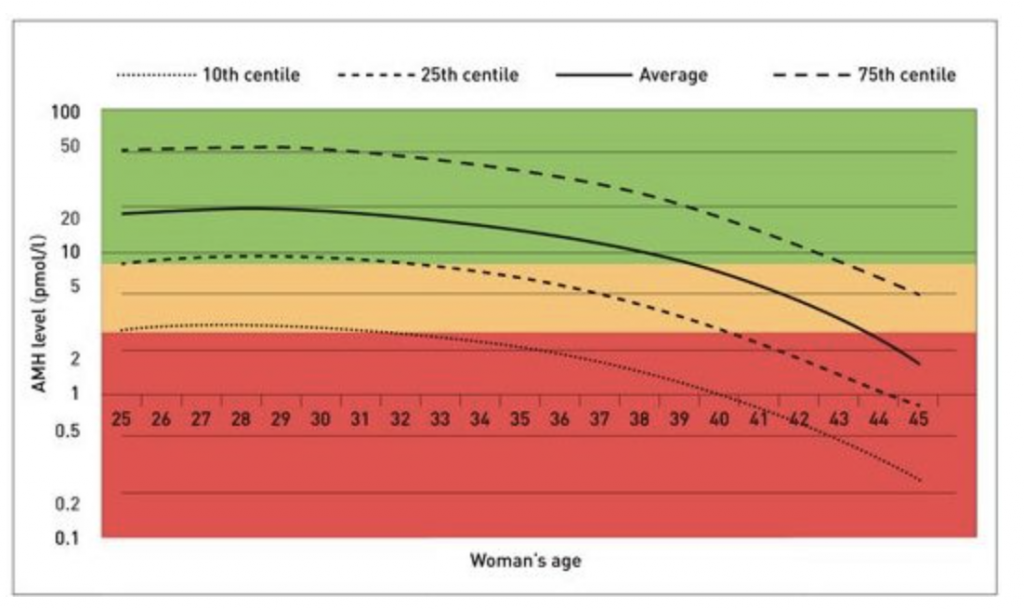
Both of our experiences have unfortunately been to learn that we are at the bottom of the chart. It’s not fun to learn this, but it’s valuable information telling us it’d be important to begin fertility treatment sooner rather than later to preserve or use what we do have left.
Why is there so much focus on the number of eggs?
Fertility is basically a numbers game. As you get through each “stage” of the process—whether harvesting eggs to freeze or turn into embryos—there’s a drop off in numbers, so you want to start with a high number if possible:
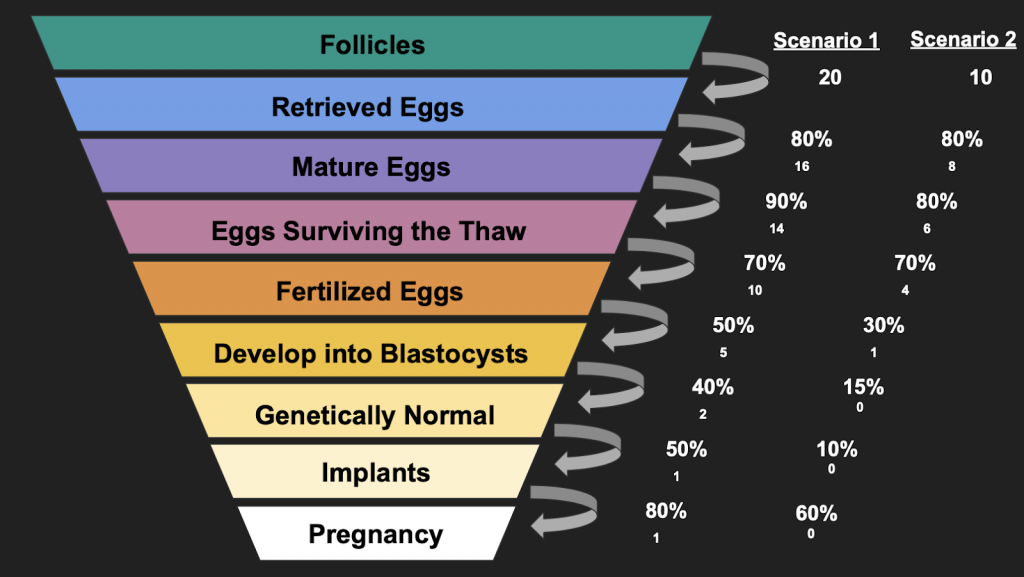
What this shows is that, statistically, starting with 20 eggs retrieved (Scenario 1, a hypothetical 30 year old) is reasonably likely to lead to 1 pregnancy. Starting with 10 eggs (Scenario 2, a hypothetical 40 year old) is much less likely to lead to pregnancy. In Scenario 2, the 40 year old may need to undergo multiple cycles to increase the chances statistically of having a pregnancy.
Keep in mind these are all statistical averages. One of the authors has had success multiple times with numbers way lower than this.
This is stressful! Why are you making me think about this now, before I even have a partner or feel ready for kids?
We’ve known so many women who discovered the above charts too late in life, and they resent that no one shared these hard truths with them when they were younger and could’ve taken action.
Here’s the crux of it: fertility only gets harder and more expensive as time goes on.
If egg freezing (for instance) is something you’re considering, know that it is way cheaper to do it at age 30 vs age 40. When you take into account the cost and probability of success at each age, it’s 90% cheaper. What a deal!
We should point out that egg freezing at age 30 (or any age) is not a guarantee or even terribly good insurance. There is a notable lack of data on success of frozen eggs, and indeed you can likely count on some of your eggs not even surviving thaw.
We recommend asking your clinic for their success rates with frozen eggs and anything else they can tell you before getting started. But all that said, egg freezing remains the best technology available today to preserve your fertility.
The cost is not small—financially, emotionally, or physically. We don’t want to minimize this. But having gone through infertility, childbirth, and the aging process, in our experience we decided it was worth the investment.
In conclusion…don’t procrastinate!
Each person needs to determine what the right path forward is for themself. We mainly want to urge you not to kick the can down the road—engage with this topic, ensure you’re informed, and make a conscious decision.
With many tech companies, and even companies like Starbucks, now offering fertility coverage, the cost of taking action is going down for many, while the cost of inaction can be surprisingly high.
Further Notes
For those who enjoy nerding out on data, here’s how we came up with the expected value calculation. Below are probabilities for two different women, both with the goal of having one child.
- Age 30:
- At normal AMH levels, let’s say you get 25 mature follicles – a “typical” result for your age.
- Applying average “conversion” rates at each step of the process, there’s a very good chance at least one of the follicles will result in a live, healthy birth. Let’s call this probability 95%. (We’re assuming here that with 25 follicles, you’ll get enough embryos for multiple months of transfers, understanding that the average success rate per month or per transer is lower than 95%.)
- The expected value of this process is the probability of a live birth (95%) times the number of cycles (1) = .95 babies.
- Clearly, you can’t have 95% of a baby, but what this means is if you did the process more than once, your expected value is additive for each additional cycle. Two cycles would give the expected value of 1.9 (.95 + .95) babies.
- Age 40:
- At normal AMH levels, let’s say you get 8 mature follicles – a “typical” result for your age.
- Applying average “conversion” rates at each step of the process, there’s a lower chance at least one of the follicles will result in a live, healthy birth. (Not only are you starting with fewer follicles, you will likely have higher drop off rates when testing for egg quality.) Let’s call this probability 10% (again, we are looking at cumulative odds rather than a single month/transer snapshot).
- The expected value of this process is the probability (10%) times the number of cycles (1) = .1 babies.
- If you did 5 cycles, you’d have an expected value of .5 babies – or a 50% chance of having a healthy, live birth.
The other factor here is cost. There are two types of cost:
- Actual dollars. At $20k a cycle:
- Age 30: $20K per cycle (plus storage for 10 years @$600/yr) = $26,000 for a very high probability (95%) of having a baby.
- Age 40: $20K per cycle (no storage, assuming immediate use) = $100,000 for a 50% chance of having a baby.
- Your time. Each cycle is about 3-4 weeks of shots, doctors appointments, feeling bloated, feeling hormonal, having restrictions on exercise, alcohol, sex, etc. Most doctors require you to “sit out” a month between cycles.
- Age 30: 1 month for a very high probability (95%) of having a baby.
- Age 40: 9 months (5 months on, 4 months “off” between cycles) for a 50% chance of having a baby.
Looking at monetary cost “per birth” (based on the likelihood of success and the costs incurred):
- Age 30:
- $26,000 to get .95 babies = $27,368 per baby
- One month to get .95 babies = 31.5 days per baby
- Age 40:
- $100,000 to get .5 babies = $200,000 per baby (assumes multiple cycles needed)
- Nine months to get .5 babies = 540 days per baby
The cost of undergoing fertility at age 30 is nearly 90% cheaper than doing it at age 40 (86.3% to be exact)! If you factor in the time element, it’s almost 95% cheaper (32 days vs 540 days).
Do you want a financial planner who can help you plan for the totality of your life, not just the money? Schedule a free consultation or send us an email.
Sign up for Flow’s weekly-ish blog email to stay on top of my blog posts and videos.
Disclaimer: This article is provided for general information and illustration purposes only. Nothing contained in the material constitutes tax advice, a recommendation for purchase or sale of any security, or investment advisory services. I encourage you to consult a financial planner, accountant, and/or legal counsel for advice specific to your situation. Reproduction of this material is prohibited without written permission from Meg Bartelt, and all rights are reserved. Read the full Disclaimer.